
MUSCULOSKELETAL INFLAMMATORY PAIN MANAGEMENT WITH LOW-DOSE DICLOFENAC AND MICROPEA ASSOCIATION: TWO CASE REPORTS
C. Cavallaro1, M. Da Roit2, L. Bloccari1 | 1Functional Recovery and Rehabilitation Unit, San Martino Hospital, AULSS1 Dolomiti, Belluno; 2Quality Service, AULSS1 Dolomiti, Belluno
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
INTRODUCTION
Inflammatory pain management is a common problem representing a clinical challenge. While non-steroidal anti-inflammatory drugs (NSAIDs), such as diclofenac, are widely used, their long-term or high-dose use should be limited due to the risk of dose-dependent side effects1. Protracted pain can lead to exhaustion of palmitoylethanolamide (PEA), an endogenous molecule with anti-inflammatory, analgesic and neuroprotective properties attributable to its ability to modulate mast cells and microglia. Then, PEA administration becomes essential to restore its endogenous levels and body homeostasis2. The association of diclofenac and PEA, particularly in its micronized and ultramicronized (m/umPEA) formulations (microPEA), could represent an innovative strategy for pain relief, combining efficacy and safety. Preliminary preclinical evidence demonstrated that combining microPEA with diclofenac enhanced the analgesic effect of the latter, allowing a reduction of its effective dose3. Here we reported the cases of two patients with musculoskeletal inflammatory pain, treated with the aforementioned association.
METHODS
A 32-year-old man (case 1) and a 55-year-old woman (case 2) suffering from pain associated with previous shoulder dislocation and tendinopathy respectively, were treated with mPEA 300 mg + umPEA 600 mg (Normast® MPS microgranules) 2 sachets/day in combination with diclofenac prolonged-release tablets, at the low dose of 75 mg/day for 10 days. MicroPEA treatment was then prolonged at the same dosage for another 20 days. Throughout the treatment period, patient 1 was also managed with conservative physical rehabilitation (FKT every other day for 10 sessions) and magnetotherapy, while patient 2 performed exercises independently at home. Pain severity (Numeric Rating Scale, NRS) and blood pressure were self-monitored by patients daily. Patients’ subjective impression and clinician’s opinion about patient’s global improvement were assessed at the end of the treatment through the Patient (PGIC) and Clinical (CGIC) Global Impression of Change. Side effects (especially gastrointestinal and cardiovascular ones) were monitored during the whole observation.
RESULTS
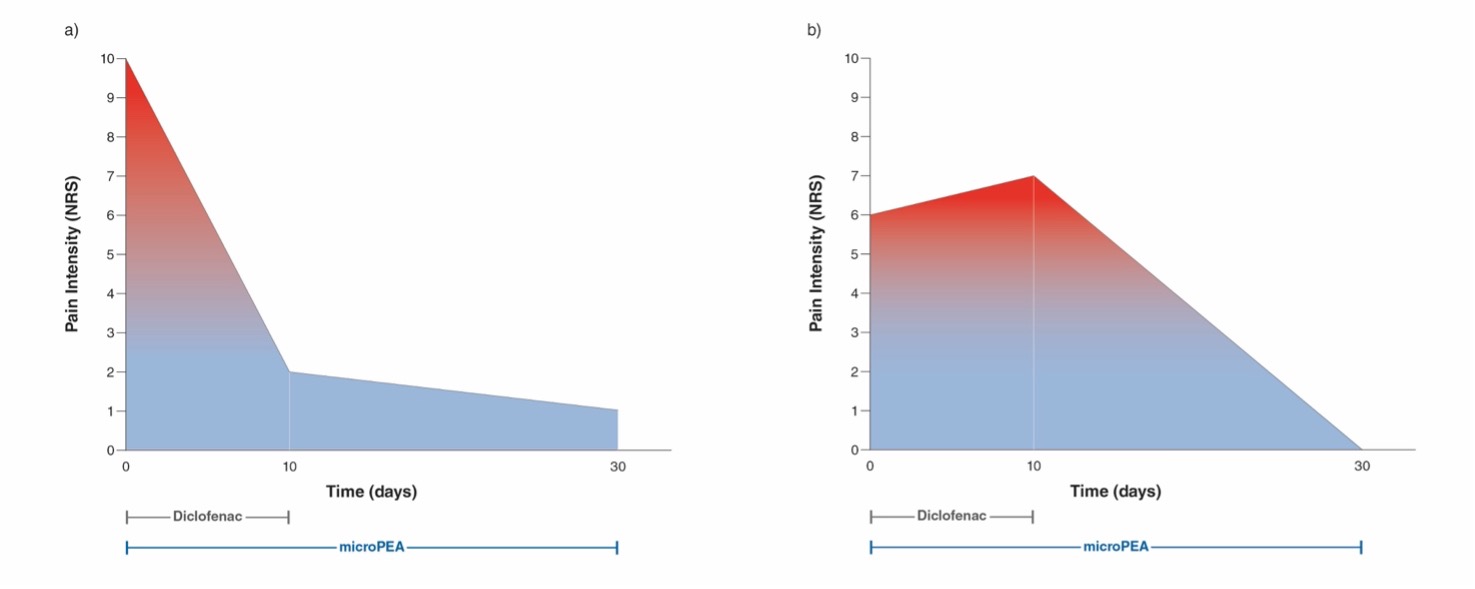
Both patients reported an evident improvement in pain. Patient 1 experienced a reduction from severe (NRS 10) to mild pain (NRS 2) after diclofenac plus microPEA treatment, further improving to a score of 1 at the end of the observation (Fig 1a). Patient 2 initially reported a slight increase in pain from moderate (NRS 6) to a score of 7 after 10 days, then achieving complete pain relief (NRS 0) at 30 days (Fig 1b). At the end of the treatment, both patients’ global status was described as "extremely improved" by their self-impressions and the clinician’s evaluation. No clinically notable changes in blood pressure were observed, and only patient 2 experienced occasionally mild gastrointestinal events throughout the observation period.
CONCLUSIONS
The association of microPEA and diclofenac effectively controlled pain, even with low doses of NSAID, minimizing its associated side effects and suggesting a probable synergistic effect. This innovative approach may offer a well-tolerated strategy for managing musculoskeletal inflammatory pain. Further research is needed to fully investigate this promising association.
Figure 1. Change in pain intensity over time Case 1 (a) and Case 2 (b).
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.