
INTESTINAL FUNGAL DYSBIOSIS AS A POTENTIAL CONTRIBUTOR TO CHRONIC LOW BACK PAIN: A CASE SERIES
J. Mendoza | Antioquia Society of Anesthesiology and Resuscitation (SADEA), Medellin, Colombia
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background and Aims. Chronic low back pain is a leading cause of disability worldwide and is commonly attributed to structural or degenerative spinal conditions. However, in many patients imaging findings do not fully explain symptom severity. Emerging evidence suggests that alterations in the gut microbiome may contribute to systemic inflammation and chronic pain states through mechanisms involving immune activation and gut barrier dysfunction.
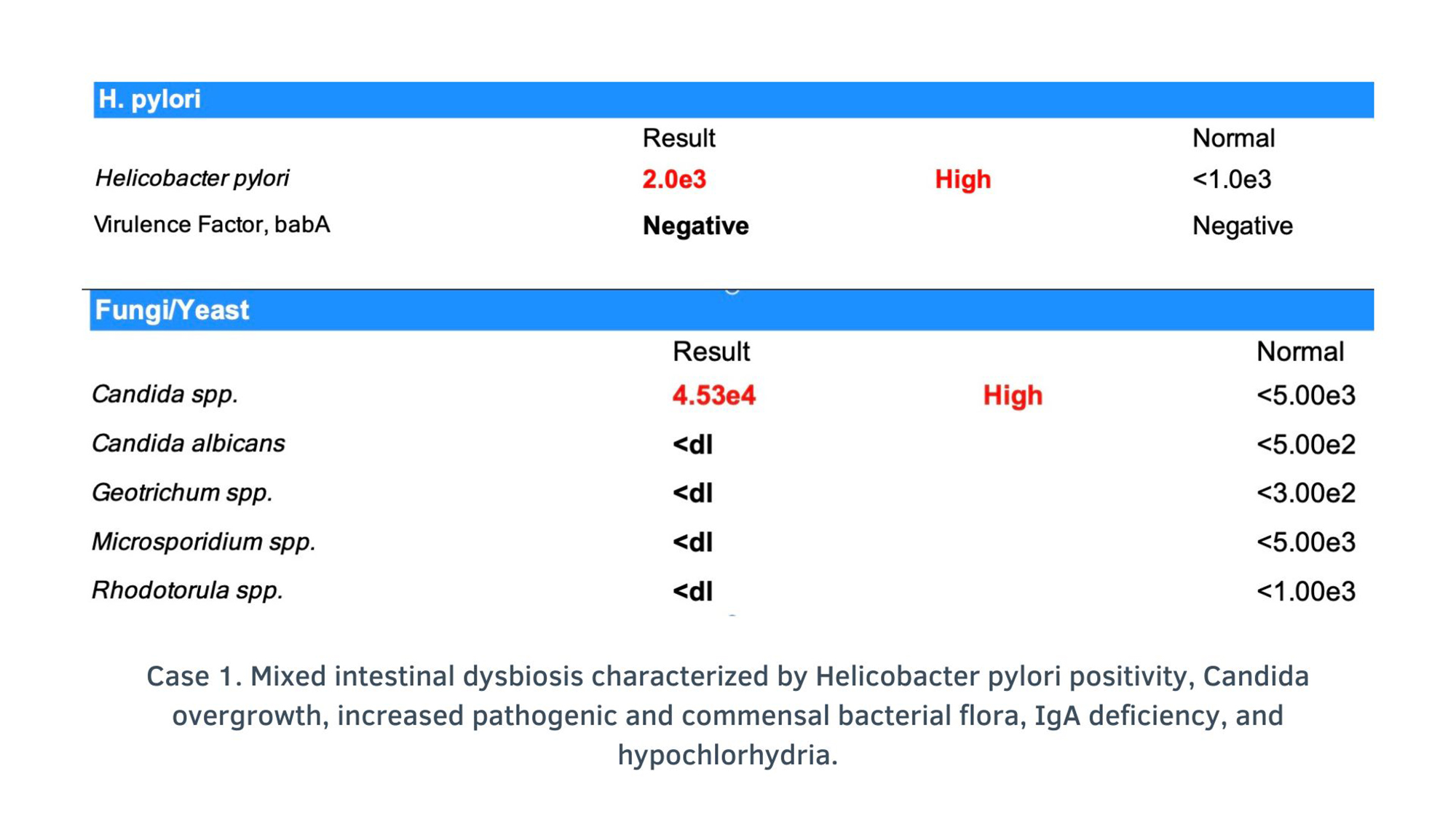
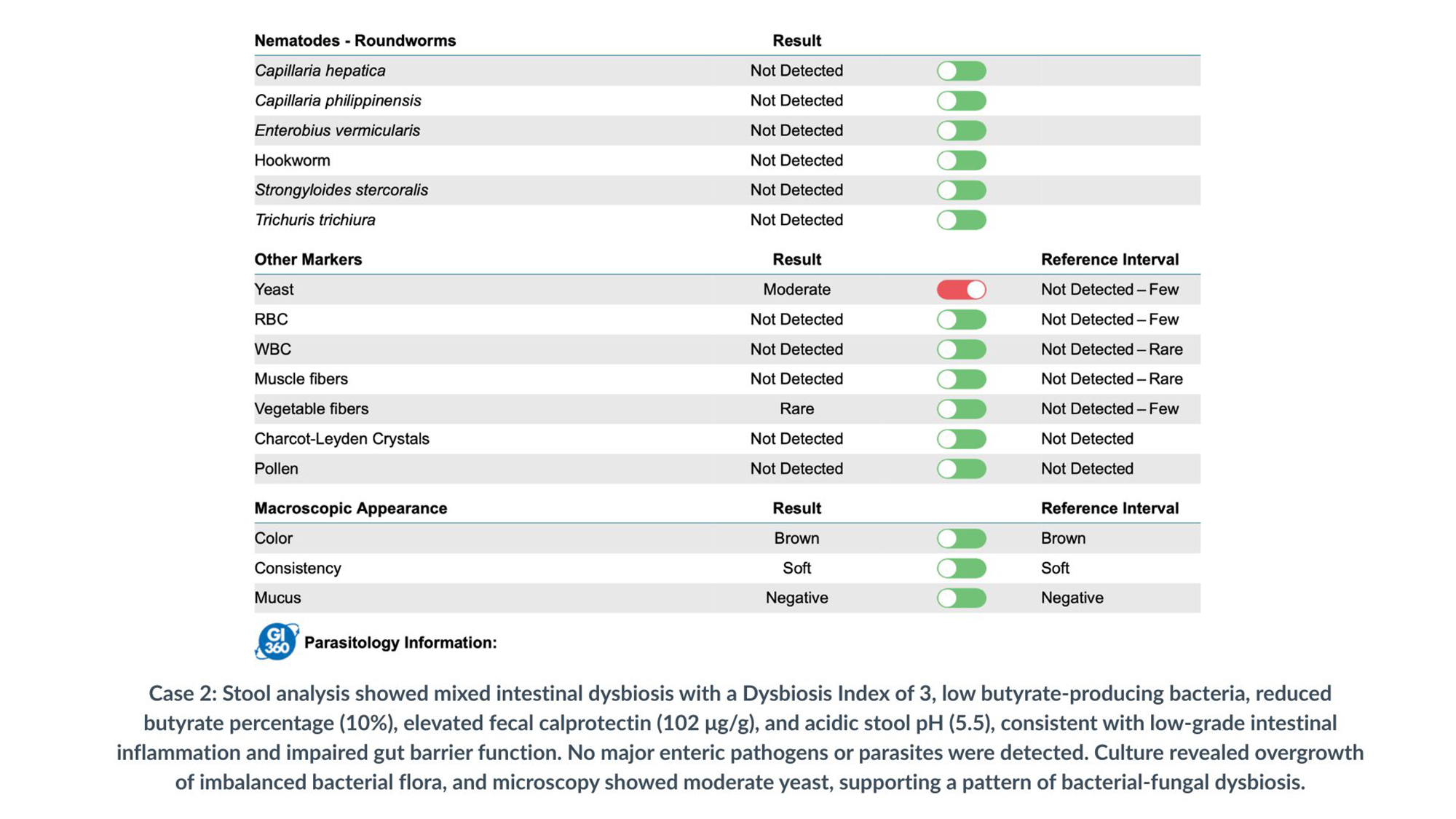
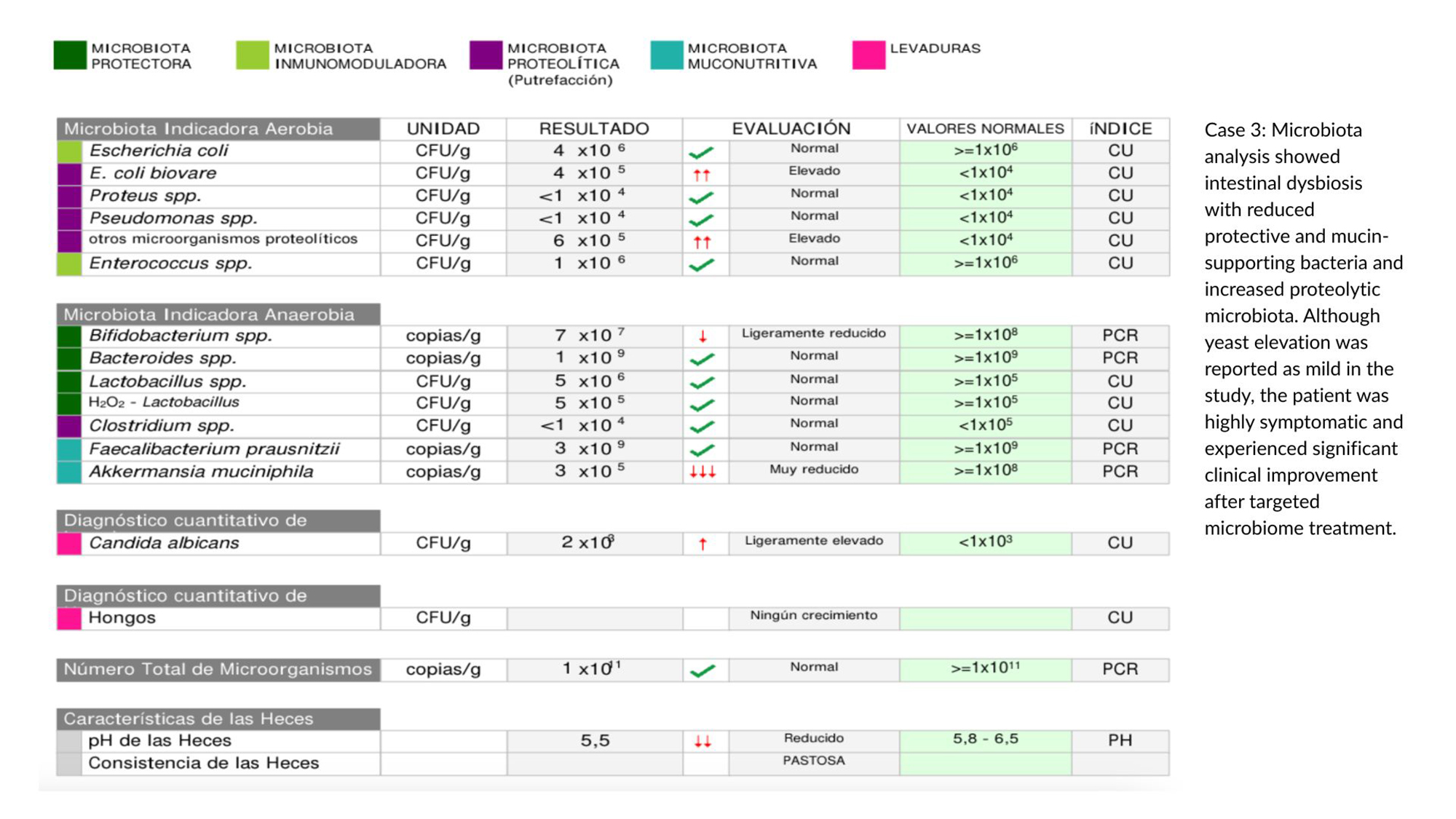
Methods. Case Presentation We report four female patients with chronic low back pain of unclear structural etiology who also presented with gastrointestinal symptoms including bloating, dyspepsia, abdominal discomfort, and altered bowel habits. All patients had persistent lumbar pain despite conventional management, including analgesics, physical therapy, and spinal interventional procedures such as lumbar facet or epidural blocks. Imaging findings demonstrated mild or nonspecific degenerative changes insufficient to explain the severity of symptoms. Microbiome and gastrointestinal evaluations revealed intestinal dysbiosis in all cases. Case 1: Mixed dysbiosis characterized by Helicobacter pylori infection, Candida overgrowth, increased pathogenic and commensal bacterial flora, IgA deficiency, and hypochlorhydria. Case 2: Stool microbiome analysis revealed mixed dysbiosis with a Dysbiosis Index of 3, decreased butyrate-producing bacteria, reduced butyrate percentage (10%), elevated fecal calprotectin (102 μg/g), and acidic stool pH (5.5), consistent with low-grade intestinal inflammation and impaired gut barrier function. Culture demonstrated overgrowth of imbalanced bacterial flora, and microscopy reported moderate yeast. Cases 3 and 4: Stool analysis reported only scarce yeast; however, both patients presented with marked gastrointestinal symptoms suggestive of fungal dysbiosis, accompanied by bacterial microbiome imbalance. Intervention. All patients underwent a microbiome-directed therapeutic protocol including an elimination diet, antifungal therapy when indicated, and microbiome-supportive supplementation aimed at restoring intestinal microbial balance and gut barrier function.
Results. Gastrointestinal symptoms began to improve around the third week of treatment in all patients. Improvement in lumbar pain occurred simultaneously with the relief of gastrointestinal symptoms. Pain intensity progressively decreased, with complete remission of lumbar pain occurring between weeks 6 and 8. Follow-up at one year demonstrated sustained remission of low back pain, persistent functional improvement, and no recurrence of symptoms.
Conclusions. This case series suggests that intestinal dysbiosis, including bacterial imbalance and fungal overgrowth, may represent an underrecognized contributor to chronic low back pain in selected patients. Evaluation of the gut microbiome may provide valuable diagnostic insights in individuals whose symptoms are not fully explained by structural spinal pathology. Clinicians should consider the possibility of microbiome-related pain mechanisms in patients presenting with diffuse or multisite pain, lumbar allodynia, and systemic symptom clusters, particularly when accompanied by complaints affecting multiple systems such as headache, cognitive impairment (“brain fog”), nasal pruritus, or gastrointestinal disturbances. These findings support the emerging concept of a gut–spine axis in chronic pain syndromes and suggest that microbiome-directed interventions may represent a promising therapeutic strategy. Further controlled studies are warranted to clarify this relationship.

Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.